
![[CIMSIGHT #5] The Unseen and Unheard: Breaking the Silence on GBV](https://cimsausu.com/wp-content/uploads/2025/12/COVER-WEB-CIMSIGHT-5.png)
Behind polite smiles and quiet streets, there are stories that go unheard. Gender-Based Violence (GBV) is not just a personal tragedy — it’s a quiet crisis, haunting countless lives around the world.
According to the WHO, 1 in 3 women globally has experienced physical or sexual violence. In Indonesia, 1 in 4 women have faced the same. While the number may seem lower, it still reveals a truth we can no longer ignore.
What Is Gender-Based Violence?
Gender-Based Violence (GBV) refers to any harmful act committed against someone because of their gender. There are many types of GBV, such as: physical and sexual abuse, emotional and economic harm, controlling behaviors and threats, human trafficking, forced or early marriage, rape, intimate partner violence, etc. GBV is rooted in inequality and abuse of power, often aimed at controlling, punishing, or devaluing individuals, especially women, girls, and marginalized gender identities.
The diagram below illustrates how Intimate Partner Violence (IPV), one of the forms of GBV, can initiate a complex chain of physical, psychological, and reproductive health consequences that may ultimately lead to long-term disability or death.
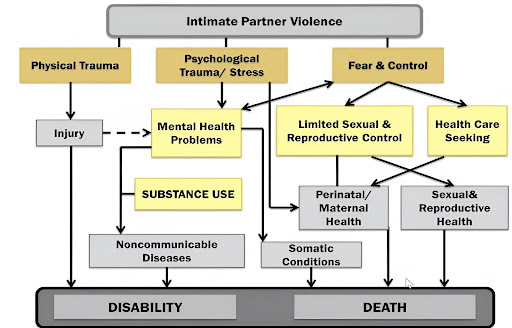
This diagram is a powerful reminder that Gender-Based Violence is not just a personal issue, but it’s a serious, life-threatening public health crisis. It shows how one act of violence can spiral into injury, trauma, disease, disability, or even death.
Problem Statement
So, to effectively address Gender-Based Violence (GBV), we must first acknowledge the systemic barriers that enable its continuation. GBV is not only rooted in power imbalances but also perpetuated by silence, stigma, and institutional neglect.
- Widespread Ignorance GBV continues to rise in part because it remains unseen or willfully ignored. Many violations happen in plain sight — in homes, schools, workplaces, and clinics — yet they are dismissed, minimized, or normalized within society.
Silenced Survivors Fear, shame, and stigma prevent many survivors from speaking out or seeking help. Even when legal protections exist, survivors often lack the support systems or social acceptance necessary to come forward safely.
Gaps in Medical Education Medical students and future healthcare professionals are rarely trained to respond to GBV with the sensitivity it requires. There is a critical gap in medical curricula regarding how to recognize, support, and care for survivors — especially when it comes to their emotional, psychological, and social needs.
DID YOU KNOW – Gender-Based Violence is one of the IFMSA Programs, which means that IFMSA underscores its urgency. GBV is a health emergency, a human rights violation, and a global responsibility.
Identifying Gender-Based Violence: Listening Between the Lines
Gender-Based Violence doesn’t always leave visible wounds. Survivors may walk into clinics with headaches, stomach pain, or fatigue, but beneath these symptoms lies something deeper. As future healthcare providers, we must learn to see what isn’t said and hear what isn’t voiced.
- Physical signs:
– Unexplained bruises, burns, and fractures
– Delayed visits for injuries - Behavioral signs:
– Fearfulness, anxiety, and depression
– Hesitation to speak in front of a partner
– Withdrawn or submissive demeanor - Verbal cues:
– Describing themselves as “controlled” or “monitored”
– Expressing guilt, self-blame, or hopelessness - Situational red flags:
– Always accompanied, never alone
– No access to money, ID, or phone
– Repeated missed appointments or canceled follow-ups - Mental health issues:
– Depression
– Panic attacks
– PTSD - Sexual & reproductive health problems:
– STIs (Sexually Transmitted Infections)
– Unwanted pregnancies - Substance use:
– Alcohol
– Tobacco
– Drug dependency Self-harm or suicidal thoughts
What Can We Do As Medical Students
- Advocacy
Advocacy is a strategic process to influence the policies, practices, or systems that affect people’s lives. It’s about speaking up, taking action, and holding decision-makers accountable. Here are the roles of medical students in advocacy :A. Amplifying Vulnerable Voices
Medical students are crucial in giving a platform to historically marginalized communities, ensuring their health needs and challenges are heard.B. Bridging Frontline to Global
They bring direct, on-the-ground perspectives from healthcare systems to international policy discussions, connecting real-world issues with global strategies.C. Mobilizing Communities
Medical students are effective in fostering awareness and catalyzing grassroots action within communities, empowering individuals to address health challenges.D. Connecting Local and Global Policy
Medical students act as vital links, translating local health realities and needs into relevant input for global health decision-making spaces.E. Driving Youth-Led Innovation
As future healthcare professionals, medical students are uniquely positioned to spearhead and implement innovative, youth-driven solutions for current and emerging health crises.Advocacy allows us to promote the rights, needs, and concerns of people who are too often ignored. Advocacy also ensures that no one is left behind during a crisis.
MHPSS (Mental Health and Psychosocial Support) dan PFA (Psychological First Aid)
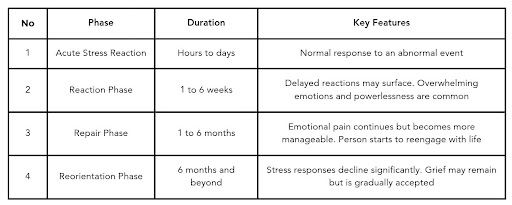
Before we explain about MHPSS and PFA, you have to know about mental health. Mental health is a state of well-being in which every individual realizes their own potential, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to their community. Mental health is a basic human right, but in many places, formal mental health services do not exist. One of the impacts of the crisis of mental health stress. There are four types of stress.
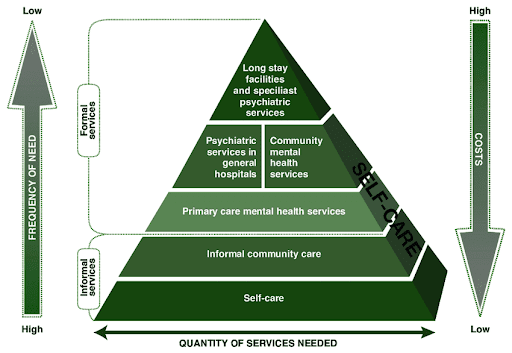
So, to solve these problems, we need MHPSS and PFA. MHPSS is any type of support that people receive to protect or promote their mental health and psychosocial wellbeing. MHPSS can range from basic essential services to specialist clinical care. Here are some forms of MHPSS.
The second one is PFA. PFA provides immediate emotional support in crises, not long term solution. The main goal is to reduce initial distress and help stabilize individuals. John Hopkins Center for Public Health Preparedness has made a structured way to provide PFA, it is RAPID.
a.) R – Rapport and Reflective Listening: build trust, convey empathy, and create a safe environment
b) A – Assessment of Needs: identify immediate physical, psychological, and social needs
c) P – Prioritization: decide which needs are most urgent and important
d) I – Intervention: provide practical assistance, emotional support, and coping strategies
e) D – Disposition and Follow-up: connect the person with ongoing support or resources if needed
Putting Survivors at the Heart of Care
There are two types of survivor-based approaches that we have to know. The first one is First-Line Support. First-Line Support is the immediate care given to a GBV survivor upon first contact with the health system. WHO defines First-Line Support using the acronym LIVES:
L – Listen: Pay close attention with empathy and without judgment.
I – Inquire: Ask about emotional, physical, and practical needs.
V – Validate: Reassure the survivor that you believe them and they are not at fault.
E – Enhance Safety: Help them create a plan to stay safe.
S – Support: Connect her to helpful information, services, or resources.
The second one is Trauma-Informed Care. Trauma-Informed Care is a set of practices that promote a culture of safety, empowerment, and healing. It includes:
- Acknowledge & Respect
Recognize the survivor’s experience and avoid repeating questions or pressuring them to recount their trauma during history-taking. - Assess Mental Health
This step is essential, and professional mental health support should be offered when needed - Physical Exam
Conduct the physical exam only with full informed consent, and ensure that only trained clinicians examine children. - Forensic Collection
Performed by a trained provider within 5 days of the assault, the exam should follow the survivor’s account and focus on collecting usable evidence, while avoiding procedures that may cause further harm (remember: virginity testing is not recommended) - Promote Safety & Support
Follow-up should be scheduled at 2 weeks, 1 month, and 3 months to monitor injuries, manage and prevent STIs, and assess mental health status.
The Role of the Health System
As future health professionals, we also need a system that empowers us to lead, serve, prevent, and act based on evidence. A strong health system plays a critical role in ending gender-based violence. So, the health system can:
- Strengthen leadership & governance on violence against women (VAW)
2. Build the capacity of health workers and improve service delivery
3. Enhance prevention programs to address gender-based violence.
4. Use evidence and data to guide decision-making
Understanding gender-based violence is more than academic, but it’s a moral imperative. This is not just about statistics or systems; it’s about lives, dignity, and the right to live free from fear. The evidence is clear: GBV leaves lasting harm. And as medical students, we are not too early in our journey to make a difference; we are right on time. Every time we choose to learn, to speak up, to support a survivor, or to question harmful norms, we are already advocating for change. Because advocacy is not just something we do — it’s something we become.
Writer : Audi Panjaitan, Dandy Azriel Silaban, Rona Uly Arzeti Siahaan (SCORP CIMSA USU)
Refrences:
Wolter, A. (2023). A novel approach to ending violence against women in Indonesia: The RESPECT framework. [online] www.who.int. Available at: https://www.who.int/indonesia/news/detail/09-11-2023-a-novel-approach-to-ending-violence-against-women-in-indonesia–the-respect-framework. Equal Measures 2030. (2024). A gender equal future in crisis? Findings from the 2024 SDG Gender Index. [pdf] Equal Measures 2030. Available at: https://equalmeasures2030.org/2024-sdg-gender-index/ UN Women (2024). FAQs: Types of violence against women and girls | UN Women – Headquarters. [online] UN Women – Headquarters. Available at: https://www.unwomen.org/en/articles/faqs/faqs-types-of-violence-against-women-and-girls. UNICEF and the Ministry of Labour and Social Welfare (MOLSW). (2021). Psychological First Aid and MHPSS Training Manual. [pdf] UNICEF and MOLSW. Available at: https://www.unicef.org/laos/reports/psychosocial-first-aid-and-mhpss-training-manual Eyosiyas Yeshialem Asefa, Assalif Beyene Haile, Osman Yimer Mohamed, and Berhanu D. (2024). The magnitude of gender-based violence, health consequences, and associated factors among women living in post-war woredas of North Shewa zone, Amhara, Ethiopia, 2022. Frontiers in global women’s health, 5. doi:https://doi.org/10.3389/fgwh.2024.1335254. Minkove, J.F. (2018). The Power of Psychological First Aid. News & Publications, Johns Hopkins Medicine, 5 April 2018. [online] Johns Hopkins Medicine. Available at: https://www.hopkinsmedicine.org/news/articles/2018/04/the-power-of-psychological-first-aid World Health Organization. (2020). Caring for women subjected to violence: A WHO curriculum for training health-care providers. [pdf] Geneva: World Health Organization. Available at: https://iris.who.int/bitstream/handle/10665/330084/9789241517102-eng.pdf World Health Organization. (2021). Global plan of action to strengthen the role of the health system within a national multisectoral response to address interpersonal violence, in particular against women and girls, and against children – Agenda item A74/21. [pdf] Seventy‑Fourth World Health Assembly, 29 May–1 June 2021, Geneva. Available at: https://apps.who.int/gb/ebwha/pdf_files/WHA74/A74_21-en.pdf |

![[CIMSIGHT #4] From Memes to Movements: How “I Choose the Bear” Sheds Light on Gender Violence](https://cimsausu.com/wp-content/uploads/2024/09/SCORP-CIMSIGHT-0-300x300.jpg)
